|

|
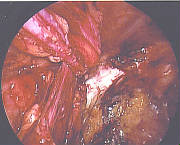
| Laparoscopic placement of mesh over the direct and indirect spaces |
|
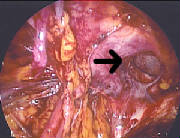
| hernia defect for a direct inguinal hernia (preperitoneal view) |
J. Douglas Reid III, MD, FACS, 3 St. Francis Dr, Suite 490, Greenville, SC 29615
J. Douglas Reid III, MD, FACS, 3 St. Francis Dr, Suite 490, Greenville, SC 29615
J. Douglas Reid III, MD, FACS, 3 St. Francis Dr, Suite 490, Greenville, SC 29615
J. Douglas Reid III, MD, FACS, 3 St. Francis Dr, Suite 490, Greenville, SC 29615
|